
Research Article | DOI: https://doi.org/10.31579/2578-8868/204
1Institute of Neurology and Neurosurgery of Cuba, Department of Neurosurgery.
2Department of Clinical Neurophysiology of the Institute of Neurology and Neurosurgery, Havana, Cuba.
3Texas Woman’s University, Department of Ph.D. Studies. Denton, TX, USA
*Corresponding Author: Norbery Jorge Rodríguez De La Paz, Institute of Neurology and Neurosurgery of Cuba, Department of Neurosurgery
Citation: Norbery Jorge Rodríguez De La Paz, Duniel A. Casas., Conceição Sallé MD, Orestes L. Piloto., Calixto Machado, Brandon Brock. (2021) Surgical Results of Lumbar Canal Recalibration by Modified Senegas Technique. J. Neuroscience and Neurological Surgery. 9(4); DOI:10.31579/2578-8868/204
Copyright: © 2021 Norbery Jorge Rodríguez De La Paz. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 23 August 2021 | Accepted: 09 September 2021 | Published: 14 September 2021
Keywords: lumbar canal stenosis; lumbar canal recalibration; modified senegas technique
The aim of recalibration of the lumbar canal using the Senegas technique guarantees stability and preserves movement, with a considerable reduction in surgical risk and faster incorporation into daily life. Objective: To evaluate the surgical results of recalibration of the lumbar canal using the modified Senegas technique.
Materials and Methods: An ambispective and cross-sectional descriptive observational study was carried out at the Institute of Neurology and Neurosurgery between January 2011 and December 2019 that were evaluated 6 and 12 months after having been operated.
Results: 70.7% of the patients manifested chronic low back pain, and dysesthesia was found in 39.8%. There were 15.8% complications. The clinical evolution according to the Lumbar and Lower Limb Verbal Numerical Scale and the functional one according to the Oswestry Disability Index was better at 6 and 12 months after the intervention compared to the preoperative period. The result was considered good at 82.7% and 89.4%, respectively, at 6 and 12 months.
Conclusions: The clinical and functional evolution of the operated patients is significantly better at 6 and 12 months concerning the preoperative one. At both 6 and 12 months, surgical results are good in the vast majority of patients.
Currently, lumbar canal stenosis is a common cause of low back pain and lower extremity pain in older adults, with an incidence of 5/100000 and a prevalence of approximately 400,000 adults in the United States 23, it is the most frequent cause of spinal surgery in patients older than 65 years, with the improvement in life expectancy and the increase in the proportion of people over 65 years of age, the incidence of will increase even more proportionally, expecting 20% by 2026. [1] In Cuba, the prevalence of lumbar spinal canal stenosis is around 6% of the population. [2]
Since the spinal canals are the roots of the nerves and the spinal cord, when a narrowing of this canal occurs, the nerve roots can be compromised, originating characteristic symptomatology consisting of pain and sensory alterations radiating to the lower limbs.
Conservative treatment is based on the use of non-steroidal anti-inflammatory drugs, physical therapy, which requires constancy and at least three months of continuity, and lifestyle changes, not always accepted by patients, and approximately 60% of cases do not resolve with that treatment. [3]
The most practiced surgical treatment until 5 or 6 years ago was decompression and posterior arthrodesis of the lumbar segment with or without instrumentation. Still, as it is not performed, immobilization in a cast brace is necessary for six months. A great limit that exists between conservative treatment and surgical, high risk. Hence, in 1988 Professor Jacques Senegas,in France, exposed his technique of systematic recalibration of the lumbar canal, by means of which the posterior arch, the articular facets, the disc, and the holes which are progressively dilated as necessary, causing minimal damage to the integrity mechanics and stability of the spine. Shortly after, he enunciated interspinous distraction as one more element of this recalibration. At the same time, he discussed a dynamic neutralization device (conservation of movement) that guarantees stability and preserves movement, significantly reducing surgical risk and faster incorporation into daily life. For this reason, the objective of the research is to evaluate the surgical results of recalibration of the lumbar canal using the modified Senegas technique. This modification proposed by us includes the endoscopic support approach as an essential tool to avoid damage to the neurovascular structures, improving the surgical field's vision. In this case, the ligamentoplasty is optional. [4]
An descriptive observational study was carried out in patients who underwent recalibration of the lumbar canal by the Senegas technique modified in the INN between January 2011 and December 2019.
The universe consisted of all the patients operated on for lumbar canal stenosis. The sample was non-probabilistic and consisted of 133 patients operated on for lumbar canal stenosis using the modified Senegas technique with the information source the clinical histories of the patients treated in the INN.
The inclusion criteria were: patients over 19 years of age, of either sex, with lumbar canal stenosis demonstrated by imaging tests (CT and/or MRI), the condition between L1-S1, the persistence of symptoms after conservative treatment for a minimum of six months, or in the presence of progressive neurological deficit.
The exclusion criteria were: patients with tumor or pseudotumoral pathology associated with the affected level, patients who underwent surgery at the level of the lumbar spine, spondylolisthesis greater than 25% slip, lateral listhesis greater than 4 mm, non-degenerative causes of stenosis, lateral curves greater than 20º associated with a degenerative process (associated scoliosis> 20º), psychiatric diseases that do not allow the functional evaluation to be carried out.
The variables studied were: age, sex, time of evolution, affected level, symptoms, signs, intraoperative complications, postoperative complications, Lumbar Verbal Numerical Scale (VNS), VNS lower limbs, Index of Oswestry Disability (ODI) and Surgical Outcomes.
The source of information was the patient's medical history. The clinical information was collected in collection charts and were included in a data collection worksheet.
The variables under study were expressed according to their respective summary measures as the arithmetic mean, standard deviation, median, interquartile range, minimum and maximum for the quantitative ones, and numbers and percentage for the qualitative ones.
To identify the association of the quantitative variables, the JI test of independence and the correlation coefficients (Pearson, Spearman), were used. For qualitative variables, t-test test was used to compare means and medians.
Final evaluation
The patients were evaluated 6 and 12 months after being operated on. The measurement of both lumbar and lower limb pain was performed using the Verbal Numerical Scale (VNS) and functional assessment using the Oswestry Disability Index (ODI).
To estimate the results of surgery at 6 and 12 months, the Macnab classification was used, which considered the result as:
Ethical considerations
The study was carried out according to the Declaration of Helsinki, modification of Fortaleza, Brazil, on research on human beings. For this, authorization was requested from the Neurosurgery service to access the clinical records, and the database of the patients included in the study, with the responsibility and obligation not to disclose the information collected, keeping it strictly confidential
The age of the patients ranged between 35 and 78 years, with a mean of 66.32 ± 8.98 years and a predominance of cases between 60 and 69 years with 52 (39.1%). A total of 84 (63.1%) patients were male. 67.7% (n = 90) of the cases had more than 12 months of disease evolution, with a median of 21.80 ± 6.11 months, minimum of 5 and 43 months maximum. The most affected levels were L4-L5 in 47.4% (n = 63), L5-S1 in 30.1% (n = 40) and L3-L4 in 15.8% (n = 21).
The symptoms referred by the patients were chronic low back, radicular pain continuous or intermittent and neurogenic claudication, dysesthesia, hypoesthesia, hyporeflexia and motor deficit. (Table 1).

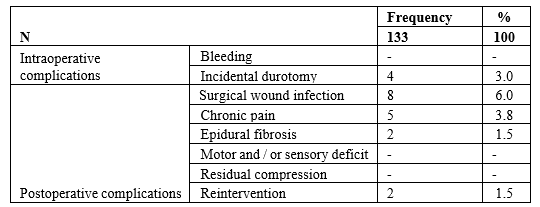
There were a total of 21 complications (Table 2), that was presented intraoperatively and consisted of injury to the dura mater, the remaining ones occurred postoperatively and surgical wound infections, chronic pain, and epidural fibrosis and reoperation, respectively.
Regarding the clinical and functional evolution of the patients studied (Table 3);
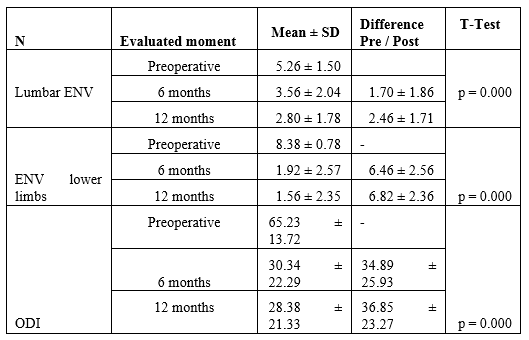
Surgical results, at six months postoperatively, were good in 110 (82.7%), fair in 19 (14.3%) and poor in 4 (3.0%), and at 12 months, they were good in 119 (89.4%), fair in 14 (10.6%) and foul in none, significant results have been statistically analyzed (Table 4).

There is a worldwide consensus that spinal canal stenosis occurs mainly between the fifth and sixth decades of life, [5] these results are consistent with those of this and other investigations [6,7] and they are explained because as people age the ligaments of the spine thicken and harden (a process called calcification), bones and joints are deformed forming osteophytes and hernias or disc protrusions commonly appear, in addition to spondylolisthesis, all factors that lead to lumbar canal stenosis. [8]
As observed in this and other studies, most lumbar canal stenoses begin with a segment, with L4-L5, followed by L5-S1, being the most affected because they are the ones that receive the most significant load and due to the accumulation of microtraumas, which favors the development of degenerative processes. As the disease becomes progressive, it secondarily affects other, generally higher segments, becoming multisegmental, and although some patients present the method in several segments from the onset of the disease, this is not the rule. [9]
The clinical presentation of lumbar canal stenosis is generally given by chronic low back pain, radiculopathy, and intermittent non-vascular claudication. The clinical symptoms in the patients included in this series are similar to those published in the literature. Lower limb pain is present in approximately 70 to 80% of patients, while low back pain is present in 60% to 65%. [10] This also has mechanical characteristics, long evolution and is accompanied by poorly defined and sometimes changing neurological symptoms in the lower extremities. Although the clinical examination of the lumbar spine usually provides little data, motor deficits that are not observed with the patient at rest can be found frequently, as well as symmetrical reduction of reflexes and some loss of sensation. Complications derived from decompression surgery for lumbar canal stenosis range between 15-30
The main limitation of the present study is its ambispective design, which means that when data are collected from medical records, there may be errors in their interpretation.
Our study shows that the complications derived from this technique are within the range described in the literature for patients who receive decompression of the lumbar canal, with a significantly better clinical and functional evolution of the operated patients at 6 and 12 months concerning the preoperative. Both at 6 and 12 months, the surgical results were rated as good in most patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
